
135 results
Removal of Hg(II) from an Aqueous Medium by Adsorption onto Natural and Alkyl-Amine Modified Brazilian Bentonite
-
- Journal:
- Clays and Clay Minerals / Volume 59 / Issue 6 / December 2011
- Published online by Cambridge University Press:
- 01 January 2024, pp. 568-580
-
- Article
- Export citation
ARIPIPRAZOLE-INDUCED OCULOGYRIC CRISIS (ACUTE DYSTONIA)
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1009-S1010
-
- Article
-
- You have access
- Open access
- Export citation
“Asking for help, quite a challenge”. Time from onset of symptoms to consultation with a psychiatrist
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S469-S470
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
One of the biggest challenges for primary care professionals is to know when it is appropriate to request a consultation with a psychiatrist. A complete medical history should be performed to detect anxious-depressive symptoms, as well as to determine the intensity, the trigger, time of evolution, and the functional repercussion (1). It is also important that the patient is able to express his or her symptoms and ask for help. The concept of “Alexitimia” refers to the difficulty of expressing feelings verbally, and is a frequent symptom in depressive patients (2).
In mild cases and with little repercussion, the physician himself can initiate treatment and follow up (3). However, on other occasions, it will be advisable to request a consultation with psychiatry.
ObjectivesThe main objective is to observe the time that elapses from the onset of symptoms until consultation with the Mental Health team is finally requested. Some preliminary results can already be obtained from this data collection.
MethodsWe have decided to carry out a descriptive study, collecting different variables from patients attending a first Psychiatry consultation.
ResultsIn a total sample of 208 patients, the majority (67%) were between 31 and 60 years old. Following the DSM-V criteria (4), patients were classified into groups according to their disorder: Adaptive, depressive, or other. These data were cross-referenced (Figure 1).
Subsequently, the time elapsed from the onset of symptoms (referred by the patients) was collected, until the referral to Psychiatry was processed. In order to make a comparison, average time (in days) was calculated for the different groups according to their age and diagnosis.
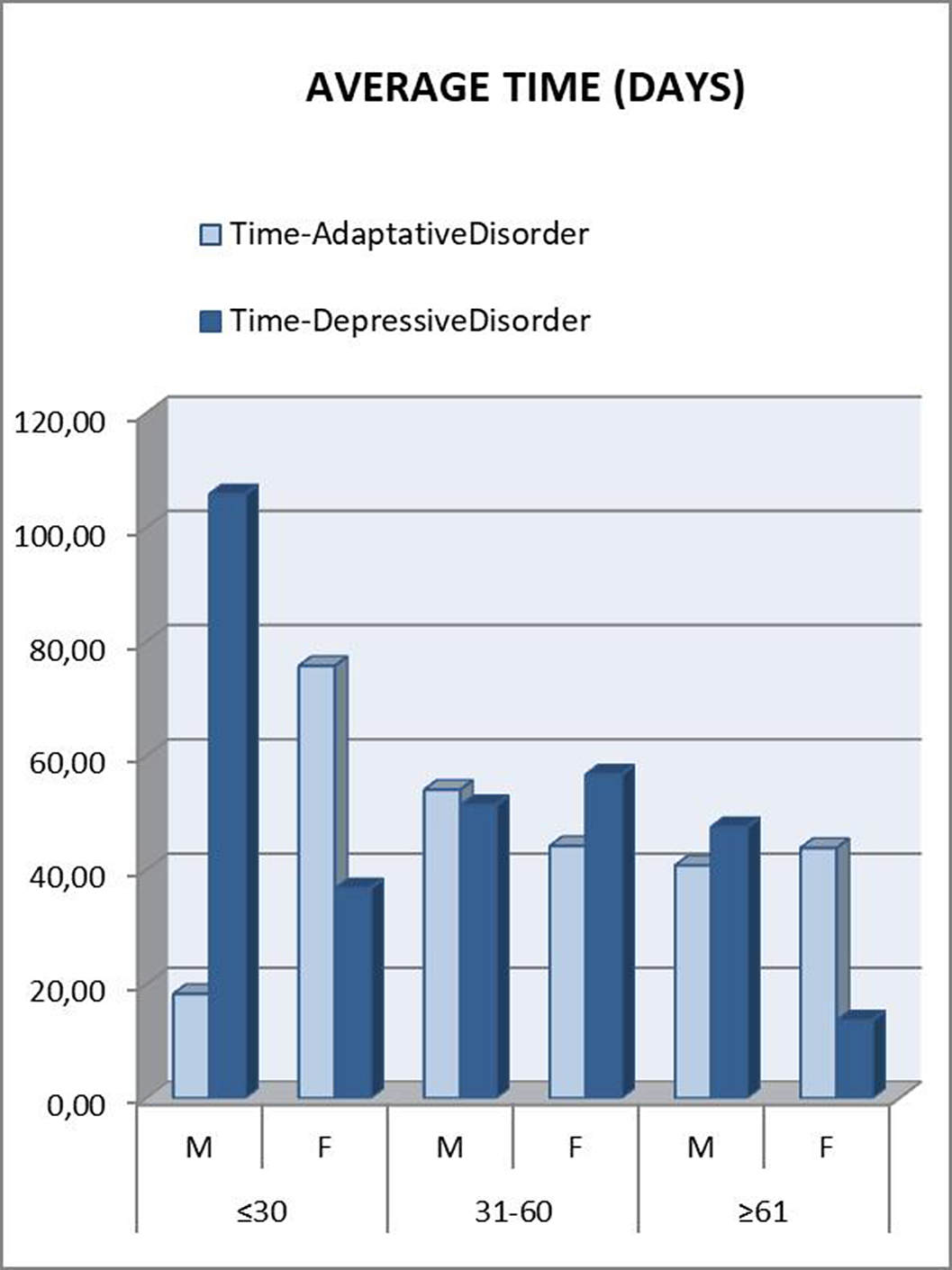
Those patients under 30 years were referred to psychiatry later. A downward trend was seen as the age range increased. In the “younger than 30” and “between 31 and 60” groups, patients who met criteria for Depressive Disorder took longer to be referred, which was striking considering that they are usually considered as more severe patients (Figure 2). This can be attributed to a greater difficulty in expressing their emotions (alexithymia), as another depressive symptom. Disaggregating these data by gender, the patients who clearly took the longest to be referred were men under 30 years old with a final diagnosis of Depressive Disorder (Figure 3). This gender difference is consistent with the social impact of alexithymia according to some articles (5).
Image:
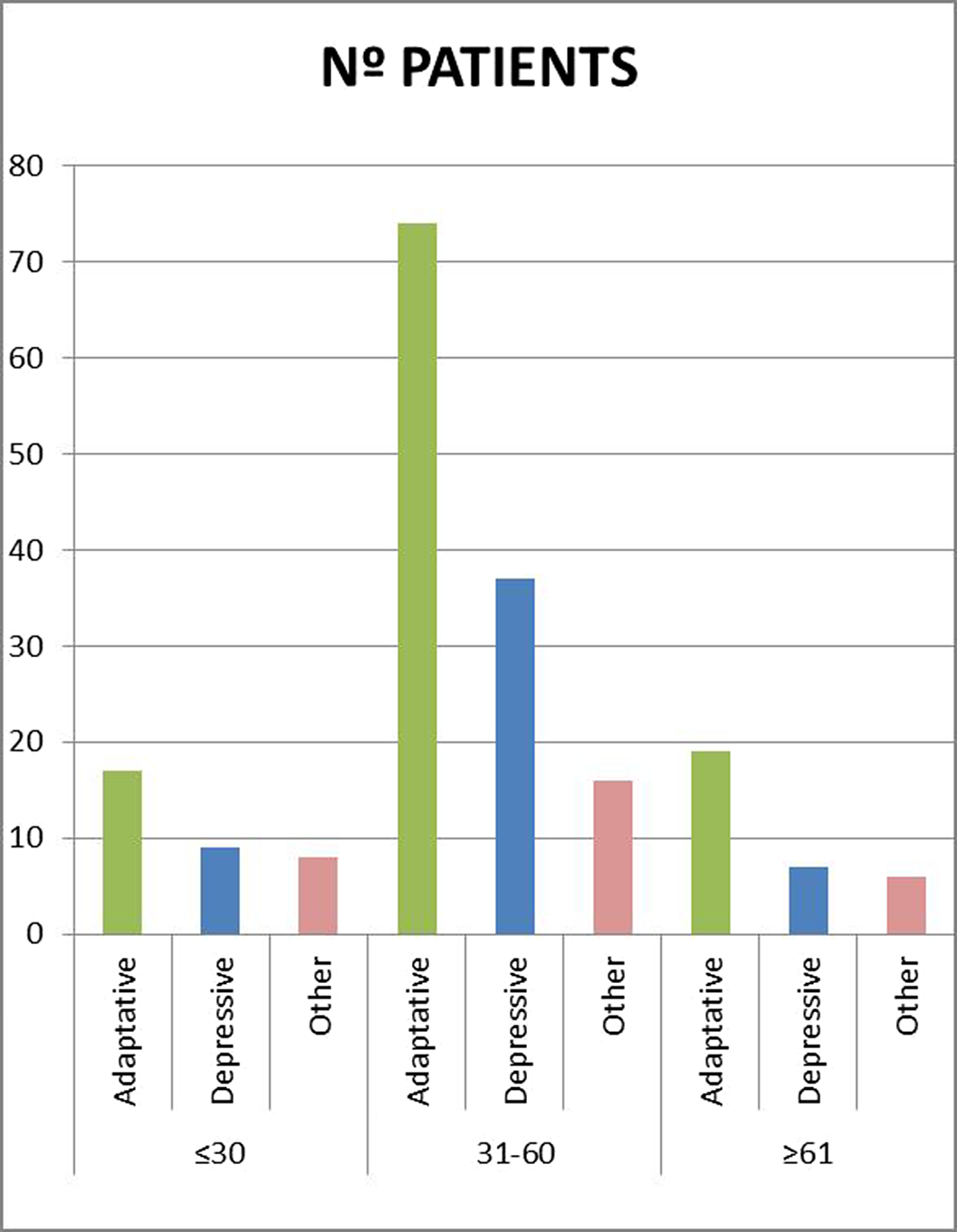
Image 2:
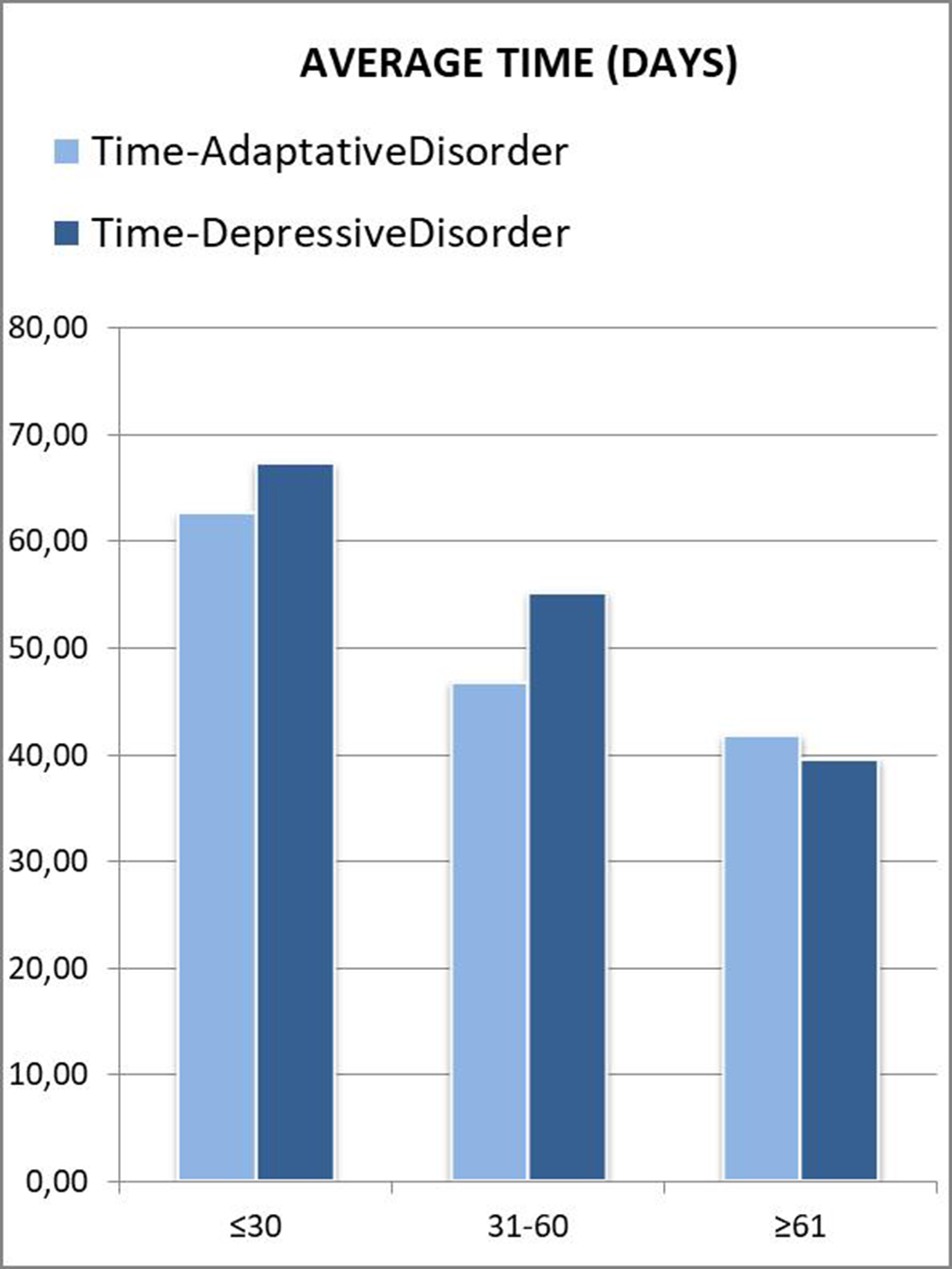
Image 3:
 Conclusions
ConclusionsIt is important that primary care physicians know how to take a complete history in those patients with symptoms of anxiety and depression.
In many cases, patients themselves have difficulties expressing their emotions and feelings (alexithymia), which may be another symptom of their discomfort.
This may lead to a delay in the time until referral to a psychiatry is requested, and therefore a worsening of symptoms.
Disclosure of InterestNone Declared



DOCTOR, I’M PREGNANT. Psychopharmacological treatment of depression in pregnant women. A clinical case of a pregnant woman and major depressive disorder
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1011
-
- Article
-
- You have access
- Open access
- Export citation
Late-onset schizophrenia: a differential diagnosis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1071-S1072
-
- Article
-
- You have access
- Open access
- Export citation
Efficacy of maintenance electroconvulsive therapy in recurrent depression: a case series
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S832
-
- Article
-
- You have access
- Open access
- Export citation
UNTIL IT BURSTS OR ALL OF US BURST. A SCHIZOTYPICAL CASE.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S967
-
- Article
-
- You have access
- Open access
- Export citation
Postictal psychosis in a psychiatric pacient, about a case
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S616
-
- Article
-
- You have access
- Open access
- Export citation
Delirious episode secondary to rotigotine: the psychotic patch
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S626
-
- Article
-
- You have access
- Open access
- Export citation
Bipolar disorder and substance use: Risk factors and prognosis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S704
-
- Article
-
- You have access
- Open access
- Export citation
I don’t know where I’m going or where I come from. Self-disorders in schizophrenia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1069-S1070
-
- Article
-
- You have access
- Open access
- Export citation
PEAKS AND VALLEYS: BIPOLAR DISORDER, RAPID CYCLERS AND ENERGY DRINKS CONSUMPTION
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S702-S703
-
- Article
-
- You have access
- Open access
- Export citation
Late diagnosis of attention deficit hyperactivity disorder and cocaine abuse
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S335-S336
-
- Article
-
- You have access
- Open access
- Export citation
Memory complaints and quality of life in a patient with mild cognitive impairment
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S937-S938
-
- Article
-
- You have access
- Open access
- Export citation
Specific treatment for alcohol use disorder reduces relapse after psichiatric hospitalization
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S565
-
- Article
-
- You have access
- Open access
- Export citation
Delusional disorder during pregnancy. A case report.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1070-S1071
-
- Article
-
- You have access
- Open access
- Export citation
“We weren’t used to seeing our colleagues hospitalized”: A clinical-qualitative study on reports from an intensivist clinical team at a Brazilian university public hospital
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S787
-
- Article
-
- You have access
- Open access
- Export citation
“The cat and the calcium”. A case of delirium secondary to hypercalcaemia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S946-S947
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Interconsultation with the psychiatry service is frequently requested from other specialties for the assessment and treatment of patients who present neuropsychiatric symptoms secondary to organic alterations. On the other hand (and in relation to this case), within the possible causes for the elevation of calcaemia figures, the most frequent are hyperparathyroidism and neoplasms, representing between these two entities 90% of cases (1).
Among the organic mental disorders, Delirium stands out, with an approximate prevalence between 1 and 2% (general population), which increases in hospitalized and elderly patients (2).
ObjectivesPresentation of a clinical case about a patient with delirium secondary to hypercalcemia, with hallucinations and behavioral disturbance.
MethodsBibliographic review including the latest articles in Pubmed about delirium (causes and treatment) and hypercalcaemia secondary to neoplasms.
ResultsWe present a 52-year-old male patient, who went to the emergency room accompanied by his wife, due to behavioral alteration. Two days before, he had been evaluated by Neurology, after a first epileptic crisis (with no previous history) that resolved spontaneously. At that time, it was decided not to start antiepileptic treatment.
The patient reported that he had left his house at midnight, looking for a cat. As he explained, this cat had appeared in his house and had left his entire bed full of insects. His wife denied that this had really happened, and when she told the patient to go to the emergency room, he had become very upset.
As background, the patient used to consume alcohol regularly, so the first hypothesis was that this was a withdrawal syndrome. However, although the consumption was daily, in recent months it was not very high, and at that time no other symptoms compatible with alcohol withdrawal were observed (tremor, tachycardia, sweating, hypertension…).
We requested a general blood test and a brain scan. The only relevant finding was hypercalcaemia 12.9mg/dL (which could also be the origin of the previous seizure). It was decided to start treatment with Diazepam and Tiapride in the emergency room, with serum perfusion, and keep under observation. After several hours, the patient felt better, the hallucinations disappeared, and calcium had dropped to 10.2mg/dL. A preferential consultation was scheduled, due to suspicion that the hypercalcaemia could be secondary to a tumor process.
Image:
 Conclusions
ConclusionsIt is important to rule out an organic alteration in those patients who present acute psychiatric symptoms. Hypercalcaemia is frequently associated with tumor processes (1) due to secretion of PTH-like peptide (4), so a complete study should be carried out in these cases.
Delirium has a prevalence between 1 and 2% in the general population (2).
Psychopharmacological treatment is used symptomatically, with antipsychotics (3). For the episode to fully resolve, the underlying cause must be treated.
Disclosure of InterestNone Declared

“Keeping an eye on amylase”. Side effects of antidepressants
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S831
-
- Article
-
- You have access
- Open access
- Export citation
My stomach is full
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S583
-
- Article
-
- You have access
- Open access
- Export citation
